
FAQs
Q: Do all staff in Joint Commission accredited programs require competency assessment, or are staff such as those in finance and human resources excused from this requirement?
A: Competency assessment is required for staff members that provide care, treatment, or services (HRM.01.06.01). Staff in the positions that are non-client facing such as billing staff, facilities maintenance staff, human resources staff, executive positions, etc. are still considered to be providing services that impact client care and thus require competency assessment. The Joint Commission standards do not differentiate between "direct" and "non-direct" care staff, rather whether staff provides care, treatment, or services for clients. Along the same lines, organizations can define expectations of contracted services and monitor the expectations per LD.04.03.09.
This information is based on guidance received from the Standards Interpretation Group (00174162 1123BIRMH672130-1)
Q: What is the dollar value “CUT-OFF” for Gifts that are not acceptable?
A: Federal regulations do not specify a dollar amount for gifts that cannot be accepted by healthcare professionals. However, some states and licensing boards do set specific dollar amounts, so you should be sure to check your local policy and seek guidance from your local Compliance & Quality Officer. For example, the Behavior Analyst Certification Board Ethics Code prohibits BCBAs and RBTs from accepting gifts valued at more than $10. Our organization’s Code of Conduct Manual provides some guidelines to help staff make informed decisions about gift giving and receipt.
Gifts shall not influence the decision-making or actions that affect the Company or clients.
Gifts should not be excessive in value, should not surpass a nominal value, nor surpass fair market value for a service.
Gifts provided by staff should not be cash, gift certificates, or “cash in kind.”
Gifts cannot be construed as a bribe, payoff, or kickback.
High risk gift scenarios include gift exchanges with clients, client family members, physicians, and referral sources. These scenarios should be approached with extra caution and guidance should be sought.
All gifts should be reported in order to ensure staff can receive guidance when needed and in order to demonstrate our organization’s commitment to ethical gift exchanges. You can access the gift reporting portal HERE. For more information on gift exchanges, access the Code of Conduct Manual or contact compliance@vivantbh.com.
Q: What is the performance cut off for calculating a healthcare disparity?
A: The standards from The Joint Commission do not provide a cut off number for what performance variance constitutes a healthcare disparity. It is possible that the interpretation of the standard during your survey will be reliant on if you can prove that the number you use is based on research and not just made up. AHRQ has conducted research in which they set their index at 10% (“The relative difference between the priority population group and the reference group must be at least 10% when framed positively or negatively”). So let’s keep the analytics simple for now and say that if a group is performing worse than a reference group by 10% of the reference group’s value, then you have likely detected a disparity. A list of typical reference groups is provided at the bottom of this answer.
Example #1
If your rate of restraint is 5 per 1000 patient days for your reference group, you calculate your disparity index by multiplying 5 by 10% (or 0.1). 5 x 0.1 = 0.5. So, 0.5 is your index (your performance range). You take your index and add it to your reference group’s performance value (as a higher value would be poorer performance for this indicator). Therefore, if another group at your program has a rate of restraint higher than 5.5, you have likely detected a disparity.
Example #2
Your average waitlist time for males (reference group) is 15 days. You want to find the disparity index for your female clients. 15 x 0.1 = 1.5. Then 15 + 1.5 = 16.5. Therefore, if female clients are waiting for more than 16.5 days, you have a potential disparity.
Example #3
Your satisfaction rating for white clients is 92%. 92 x .1 = 9.2 Then 92 - 9.2 = 82.8 Therefore, if another racial/ethnic group has a satisfaction rating below 82.8%, you may have detected a disparity.
What if I cannot find any disparities?
If you have combed your data and cannot find any disparities, reach out to your Compliance & Quality Officer to review the data in great detail. Review your data and make sure no potential indicators were missed for evaluation, then we can thoroughly document your efforts and findings. The standard says you must develop a written plan to address “at least one of the health care disparities identified in [your] patient population.” Theoretically, if you don’t find a single disparity, then you don’t have a disparity to address.
In their notes for the standard, TJC provides examples of quality/safety data to review, including treatment for SUD, restraint use, suicide rates, experience of care, and communication. They also provide examples of sociodemographic characteristics, including age, gender, preferred language, and race and ethnicity.
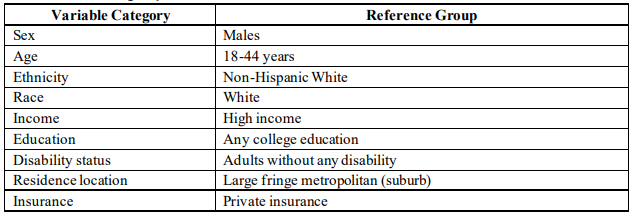
Common reference groups identified in ARHQ’s healthcare disparities reporting.
Q: Why can’t we place items in front of exit doors, even if they are easy to move?
A: Blocking exit routes creates several risks to employee and client safety as well as regulatory noncompliance. Exit routes might seem like one of the simplest parts of the workplace - just look for the glowing exit sign and head out, correct? In theory that may be true, but technically speaking, exit routes have several features required by regulators such as OSHA, Joint Commission, and state licensing, and one of those features is making sure they are always clear.
Workplace Safety
We have seen workplace fires in other countries where employees were killed because they couldn’t escape on the news, and OSHA has called specific attention to a fire at a poultry processing plant in China where over 100 workers died because exits were locked or obstructed. A nursing home fire in Australia in 2011 also resulted in 21 deaths and 80 hospitalizations, a contributing factor was exit routes being blocked by furniture. In a clear moment, it may seem like you can easily move a small table that’s in front of a door or shuffle some boxes out of the way. However, what real life scenarios have shown us is that in a smoke-filled, active fire situation, these tasks may be significantly more challenging than one anticipates.
Regulatory Noncompliance
Blocking exit doors is one of the most frequently cited environmental safety standards by organizations like OSHA and The Joint Commission. Under OSHA, organizations like Family Dollar have recently been fined over $290,000 for violating this standard. The Joint Commission may cite a violation of exit route safety as a “high risk” or “immediate threat to life” level of severity. These types of citations can risk continued accreditation and your reputation as a safe, high-quality health care provider.